

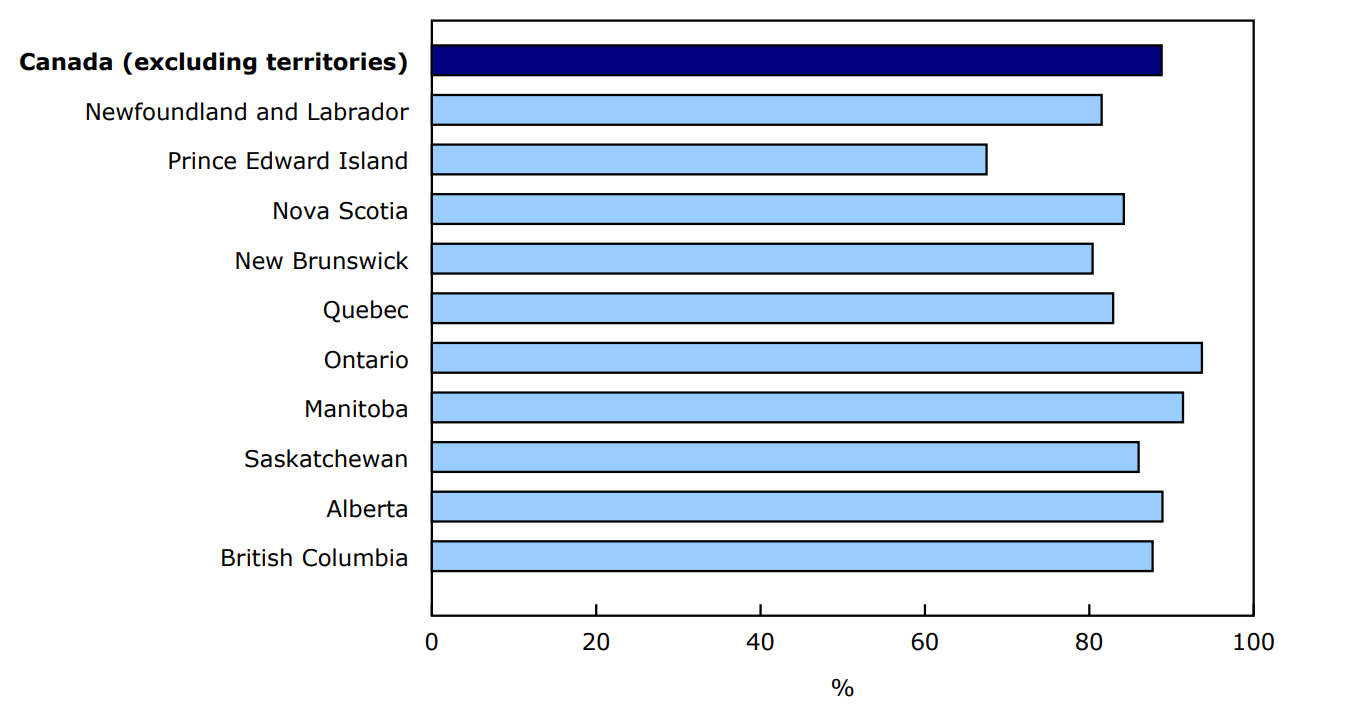
The Canadian Health Survey on Children and Youth (CHSCY) found that nearly 9 in 10 (89%) children and youth living in the provinces had a primary health care provider in 2024. The measure of Canadians with a primary health care provider is one of the Shared Health Priorities (SHP) indicators that the CHSCY is collecting, to report on children and youth aged 1 to 17 years. The SHP indicators were developed collaboratively by federal, provincial, and territorial governments in 2023, in partnership with the Canadian Institute for Health Information, to ensure health care systems continue to respond to the needs of Canadians.
The proportion of children and youth with a primary health care provider varied by province of residence for 2024, ranging from 94% in Ontario to 68% in Prince Edward Island (Chart 1). The 2023 results for access to a "regular health care provider" encompassed a wider range of health professionals, however they showed similar provincial patterns.
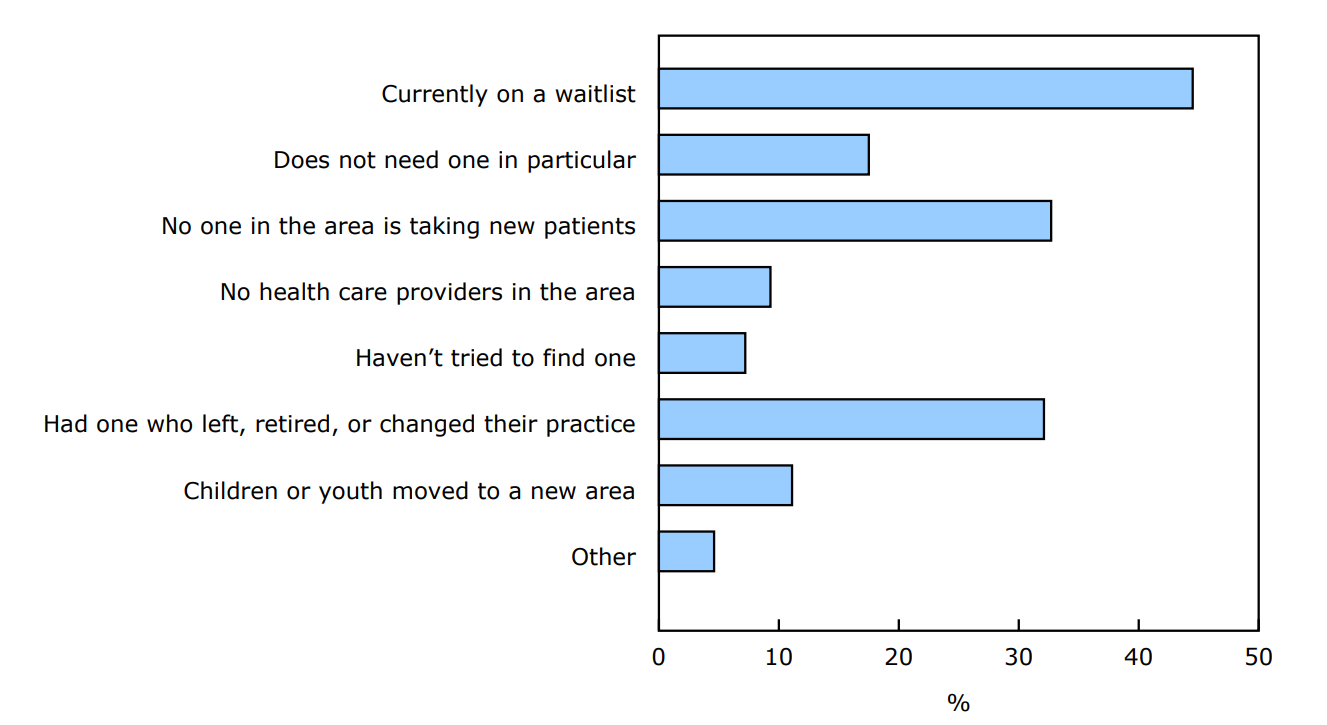
For children and youth without a primary health care provider in 2024, parents were asked to specify one or more reasons as to why they did not have one. Among the 11% of children and youth who did not have a primary health care provider, 32% were without one because theirs left or had retired, and 33% had no one in the area taking new patients (Chart 2). These responses were similar to what was reported in 2023 for those who did not have a regular health care provider.
This Daily article follows a previous release of the 2024 CHSCY SHP indicators in a table.
Over two-fifths of children and youth were able to consult a primary health care provider the same or next day
Among children and youth who had consulted a primary health care provider when they were sick or concerned about their health in the 12 months prior to the survey, 43% were able to consult a primary health care provider the same day they requested or else the next day (Table 1). Timely access to a primary health care provider is based on the last visit, and includes experiences for children and youth both with or without a primary health care provider. For those with a primary health care provider, their last visit may have been with an alternative primary health care provider. Timely access to primary health care can help prevent emergency department visits or hospitalizations for conditions that are manageable in a primary health care setting. In addition to those who were able to consult the same or next day, 40% were able to consult a provider within two days to less than two weeks, and 18% waited two weeks or more for the consultation (Table 1). Parents were also asked about their level of satisfaction with the time they had to wait between requesting care for their child, and the consultation. When asked about their satisfaction, 68% were satisfied with the wait time to consult the primary health care provider (Table 2).
The proportion of children and youth who were able to consult a health care provider the same or next day, as well as their satisfaction, varied by province (Table 2). Children and youth in Ontario (50%) had the highest proportion who were able to consult a primary health care provider the same or next day. Additionally, a higher proportion of parents in Ontario were satisfied with the wait time (72%) compared to the national average (68%). In contrast, British Columbia had the lowest proportion able to receive a same day or next day appointment (25%) and a lower proportion of parents were satisfied with the wait time (56%) than the national average.
Aspects of the primary health care system, such as its structure, delivery models, and lack of culturally safe practices, can result in care that is difficult to access and often incomplete for Indigenous people. Looking at Indigenous children and youth living off-reserve within the 10 provinces, 50% of First Nations children and youth and 26% of Métis children and youth were able to see a primary health care provider the same or next day. This was a lower proportion of Métis children compared to non-Indigenous children (43%). Additionally, a lower proportion of parents of Métis children reported being satisfied with the wait time (61% vs. 68% for parents of non-Indigenous children). Among parents of First Nations children, the proportion who reported being satisfied is comparable to that of parents of non-Indigenous children. Results specific to Inuit children were not included individually in the analysis due to an insufficient sample size which limited the ability to produce reliable estimates.
Immigrant families can face barriers such as language difficulties, cultural differences, and limited knowledge of the Canadian health system, all of which may impact their health care experience (Table 2). Results from the 2024 CHSCY show that a lower proportion of immigrant children and youth (38%) were able to consult a primary health care provider the same or next day when sick or concerned, compared to non-immigrant children and youth (43%). However, parental satisfaction with the wait time was similar between the two populations.
Lower proportion of children and youth with long-term conditions were able to consult a primary health care provider the same or next day
In 2024, 28% of children and youth aged 1 to 17 years had one or more long-term health condition. Just over one in three children and youth (36%) with a long-term condition were able to consult a primary health care provider the same or next day, compared to 46% for those without a long-term condition. Looking at ability to consult a primary health care provider the same or next day by type of long-term condition, the proportion is even lower among those with a diagnosed mental health disorder, with less than one-quarter of these children and youth (21%) able to consult a primary health care provider the same or next day. The proportion was 32% for children and youth with neurodevelopmental disorders and 40% for those with physical disorders.
The specific reasons children and youth with long term conditions sought primary health care were not asked in the CHSCY. Thus, it is possible that they were not seeking care for their long-term condition, but for another issue. However, for both children and youth with and without long-term conditions, factors such as the availability of services, urgency of health condition, purpose of appointment, and type of provider being consulted can have an impact on the duration of the wait time between requesting and consulting a primary health care provider.
Over 80% of children and youth with a primary health care provider received culturally sensitive care, a greater proportion than those without
In 2024, a majority (81%) of parents strongly agreed or agreed that their child or youth received culturally sensitive care. Additionally, 17% neither agreed nor disagreed, and 1% disagreed or strongly disagreed (Table 3). Parents of children and youth who had a primary health care provider had a higher proportion who strongly agreed or agreed (82%) that their child received care that was sensitive to their cultural background and identity, compared to those that did not have a primary health care provider (70%).
Discrimination and racism are documented barriers to accessing health care for Indigenous people in Canada. For the parents of First Nations children and youth living off-reserve within the 10 provinces, a lower proportion strongly agreed or agreed (71%) that their child received culturally sensitive care, compared to the parents of non-Indigenous children and youth (82%). Additionally, a greater proportion of parents of First Nations children and youth neither agreed nor disagreed (25%) with this statement, compared to the parents of non-Indigenous children and youth (17%). Similarly, compared to parents of non-Indigenous children and youth, a lower proportion of parents of Métis children and youth agreed or strongly agreed that their child received culturally sensitive care (71%) and a greater proportion neither agreed nor disagreed (27%).
Perception of whether the care received for children and youth was culturally sensitive also varied among racialized groups. Black (73%) and Arab (73%) children and youth had a lower proportion of parents who strongly agreed or agreed that their child received care that was sensitive to their cultural background and identity, compared to all children and youth (81%). In contrast, Filipino (88%) children and youth had a higher proportion of parents who strongly agreed or agreed with this statement.
Chart 1: Percentage of children and youth aged 1 to 17 with a primary health care provider, by province, 2024
Description - Chart 1
Data table: Percentage of children and youth aged 1 to 17 with a primary health care provider, by province, 2024
Source: Canadian Health Survey on Children and Youth, 2024 (5233).
Chart 2: Reasons children and youth aged 1 to 17 do not have a primary health care provider, 2024
Description - Chart 2
Data table: Reasons children and youth aged 1 to 17 do not have a primary health care provider, 2024
Source: Canadian Health Survey on Children and Youth, 2024 (5233).
Correction note
On December 16, 2025, estimates for "Canadians with same-day or next-day access to a health care provider," "Canadians who were satisfied with the wait time to access a health care provider," and "Canadians treated with respect regarding culture and identity by a health care provider" were corrected throughout the Daily release, including across all three tables.
These revisions were made to ensure the estimates align with the intended indicator definitions by fully removing those who paid out-of-pocket as part of a private pay model (i.e., individuals whose services are not covered by the public system).
Note to readers
The 2024 Canadian Health Survey on Children and Youth (CHSCY) is a cross-sectional survey covering the population aged 1 to 17 as of August 31, 2024, living in the 10 provinces and 3 territories. Children and youth on First Nation reserves and other Indigenous settlements, children and youth living in foster homes and not eligible for the Canada Child Benefit, and the institutionalized population are excluded from the CHSCY.
It should be noted that the CHSCY program is designed to produce reliable estimates at the provincial level on a yearly basis and at the territorial level on a two-year basis. While children and youth residing in the three territories were included in the 2024 collection, they are not included in this analysis. Instead, data for the territories will be reported when the combined data for 2024 and 2025 are released in 2026.
Data were collected from the parent or legal guardian about the preselected child or youth. For simplicity, the term "parent" is used in this release.
In support of the Shared Health Priorities (SHP), Statistics Canada will be collecting data from 2024 to 2027 through the CHSCY program to enable measuring and reporting on selected SHP indicators related to access to primary health care and mental health services for children and youth aged 1 to 17 years. The SHP indicators included in the CHSCY are the following:
- Canadians with a primary health care provider;
- Canadians with same day or next day access to a health care provider;
- Canadians who were satisfied with the wait time to access a health care provider;
- Canadians treated with respect regarding culture and identity by a health care provider;
- Canadians with a mental health disorder who have an unmet need for mental health care.
The response rate for the 2024 CHSCY was 30% for 1- to 4-year-olds, 31.6% for 5- to 11-year-olds and 20.6% for 12- to 17-years-olds, which resulted in 15,124 cases in the provinces. Survey sample weights were applied so that the analyses are representative of the 2024 Canadian population for children and youth aged 1 to 17 as of August 31, 2024, living in the provinces.
The term immigrant refers to children or youth who were reported by their parents as being or who having ever been, landed immigrants or permanent residents. Such persons have been granted the right to live in Canada permanently by immigration authorities. Immigrants who have obtained Canadian citizenship by naturalization are included in this category.
In this release, data on racialized groups are measured with the 'visible minority' variable. The 'non-racialized non-Indigenous group' is measured with the category 'Not a visible minority' of the variable, excluding Indigenous respondents. "Visible minority" refers to whether or not a person belongs to one of the visible minority groups defined by the Employment Equity Act. The Employment Equity Act defines visible minorities as "persons, other than Aboriginal peoples, who are non-Caucasian in race or non-white in colour." The visible minority population consists mainly of the following groups: South Asian, Chinese, Black, Filipino, Latin American, Arab, Southeast Asian, West Asian, Korean and Japanese.
Indigenous identity of the child or youth is based on the parent-reported answer to whether or not the child is First Nations, Métis or Inuk (Inuit) (self-identification). Here, First Nations (North American Indian) includes Status and Non-Status Indians. The results discussed do not include Indigenous people living in the territories, on First Nations reserves and other Indigenous settlements, who may have different experiences related to access to health care. Data on children and youth reporting having multiple Indigenous identities are included in the Indigenous total but are not shown separately because of small sample sizes.
Long-term conditions were based on a series of questions asking parents of 1- to 17-year-olds if the child has been diagnosed with any of the listed long-term health conditions, with some conditions only applying to children aged 5 to 17, or 12 to 17. Long-term conditions in this analysis were categorized into three categories: mental health disorders, neurodevelopmental disorders, and physical disorders. Mental health disorders include anxiety disorder, mood disorder (5- to 17-year-olds), eating disorder (5- to 17-year-olds), post-traumatic stress disorder (5- to 17-year-olds), obsessive-compulsive disorder (5- to 17-year-olds), oppositional defiant disorder (5- to 17-year-olds) and substance use disorder (12- to 17-year-olds). Neurodevelopmental disorders include learning disability or learning disorder (5- to 17-year-olds), autism spectrum disorder, attention deficit disorder with or without hyperactivity, epilepsy and fetal alcohol spectrum disorder. Physical disorders include asthma, diabetes, allergies and chronic pain.
Having a primary health care provider was based on a question which asked parents of 1- to 17-year-olds if their child had a regular primary health care provider they could consult with when the child needed care or advice for their health, including a family doctor, a pediatrician, a nurse practitioner or a team of health professionals. For parents who reported having a primary health care provider for their child or youth, they were asked if they needed to pay out-of-pocket for the consultation due to the provider being in a private pay model. If a parent reported paying out of pocket, they were not considered as having a primary health care provider for their child or youth. Previous results from 2023 reporting on access to a "regular health care provider" encompassed a wider range of professionals, including specialists and other health professionals.
Ability to consult a primary health care provider the same day or the next day was based on a question asking parents of 1- to 17-year-olds who reported that the child or youth consulted a primary health care provider when the child was sick or they were concerned about the child's health in the 12 months prior to the survey, how long they had to wait between the time they requested care for this child and when the child consulted the primary health care provider at their most recent consultation. This question was asked to those who reported consulting a primary health care provider in the 12 months prior to the survey when sick or concerned about their health, regardless of whether or not the parent reported that their child had a primary health care provider they could consult with when they needed care or advice for their health.
Satisfaction with wait time was based on a question asking parents of 1- to 17-year-olds who reported that the child or youth consulted a primary health care provider when the child was sick or they were concerned about the child's health, in the 12 months prior to the survey, how satisfied they were with the wait time between requesting care and consulting with the primary health care provider at their most recent consultation. Answer options included very satisfied, satisfied, neither satisfied nor dissatisfied, dissatisfied or strongly dissatisfied. Satisfaction represents those parents who were satisfied or very satisfied with the wait.
Culturally sensitive care was based on a question asking parents of 1- to 17-year-olds who reported that the child or youth consulted a primary health care provider when the child was sick or they were concerned about the child's health in the 12 months prior to the survey, to what extent they would agree or disagree that the child received health care that was sensitive to their cultural background and identity at their most recent consultation. Respondents were asked to include treatment based on age, sex, gender, sexual orientation, ethnicity, Indigenous identity, race, language, accent, religion or spirituality, disability, or other factors. Response options included strongly agree, agree, neither agree nor disagree, disagree or strongly disagree, with those parents reporting strongly agree or agree used as "received culturally sensitive care" for this analysis.
For more information on survey definitions and methods, refer to the Statistics Canada survey information page: Canadian Health Survey on Children and Youth.
Contact information
For more information, or to enquire about the concepts, methods or data quality of this release, contact us (toll-free 1-800-263-1136; 514-283-8300; infostats@statcan.gc.ca) or Media Relations (statcan.mediahotline-ligneinfomedias.statcan@statcan.gc.ca).