
Projecting the future of health in Canada using microsimulation modelling

Periodically, the StatCan Blog publishes a guest post on research at Statistics Canada. This post is from Deirdre Hennessy and Bill Flanagan, research analysts in the Health Analysis Division.
Some of the most important questions for health policy makers, planners and clinicians have to do with the future. In order to design effective prevention and screening programs, health policy makers must be able to estimate future trends in risk factors for disease and future disease occurrences. Another aspect of thinking about the future is considering alternative or "what-if" scenarios. These scenarios allow policy makers to compare and weigh the benefits and costs of different disease prevention strategies.
In general, simulation modelling approaches have been used to describe and model complex systems in the fields of economics, environmental sciences and engineering, and increasingly in health. Specifically, dynamic microsimulation modelling techniques have been gaining traction and have been used to inform policy in relation to complex health and health care system problems in many countries.Footnote 1 In Canada, organizations such as Statistics Canada, Health Canada, the Public Health Agency of Canada (PHAC), and the Canadian Partnership Against Cancer (CPAC) have employed microsimulation models to project future incidence and prevalence of risk factors and diseases, as well as future demands for health care resources.
What is dynamic microsimulation?
Dynamic microsimulation, in the context of social science and population health, is the simulation of large samples of individuals (micro) and their behaviours, states and actions over time (dynamic). The purpose is to project the socioeconomic and demographic developments of society.Footnote 2 Individuals' behaviours, states and actions are modelled using multiple sources of data including surveys, administrative databases, vital statistics and census data. This technique explicitly simulates individuals and attempts to produce a realistic set of heterogeneous health biographies over the course of an individual's life. For example, within the model, individuals' age, their health behaviours and disease states change realistically and they eventually die. Individual health biographies are summed up to present a projected portrait of the health of the Canadian population.
How can microsimulation models be useful as health policy tools?
In health policy, prevention and screening strategies have traditionally been evaluated after implementation. This approach is limited because policy makers, who know that large-scale expensive programs can sometimes fail, may be reluctant to implement them despite their potential benefits. In addition, failure or unforeseen consequences of a policy or program may only be revealed after implementation. Microsimulation modelling offers an evaluation method that allows policy makers to examine the results, consequences and benefits of a program in advance of implementation.Footnote 3 Policy makers can also use these projections to build a business case for policy change.
Application of microsimulation modelling in Canada
At a population level, simulation models inform decisions on prevention and control activities for chronic diseases, including cancer and coronary heart disease. Specifically, they can be used to compare and evaluate a wide range of intervention strategies (including prevention, early detection and screening) and therapeutic options; this helps assess strategies intended to reduce health care costs and improve health outcomes. Below we describe some of the applications of microsimulation models developed at Statistics Canada in collaboration with our partners.
Modelling cancer: OncoSim
OncoSim is a free, web-enabled, empirically grounded microsimulation tool that evaluates cancer control strategies for prevention, screening and treatment. Registered users can create and perform their own analysis by changing input parameters on the website (oncosim.ca). Provincial health ministries across the country have used OncoSim to evaluate screening strategies for cervical, colorectal and lung cancer.
For cervical cancer, alternative screening strategies evaluated the impact of raising the initial screening age from 21 to 25 as per the new guidelines, and the potential costs and benefits of switching from cytology-based screening to DNA testing for the presence of human papillomavirus (Figure 1, adapted from Papadiuk et al.Footnote 4). Also evaluated was the impact of vaccination against human papillomavirus in reducing cancer and treatment, as well as how it may influence the need for screening in the future.Footnote 5
The initial recommendations of the National Committee on Colorectal Cancer Screening in 2002Footnote 6 were informed by microsimulation projections for Canada using OncoSim's predecessor. OncoSim has been further developed to evaluate alternative screening modalities, including flexible sigmoidoscopy and colonoscopy.Footnote 7
Currently there are no organized screening programs for lung cancer in Canada, although a pilot program is underway in Ontario. To assist decision makers in Canada (provincially), a fully validated model of lung cancer screening was developed to assess the cost effectiveness, budgetary impact and resource implications of population-based screening of high-risk individuals.Footnote 8 A wide range of scenarios were evaluated by varying participation and adherence rates; age and high-risk thresholds for eligibility; frequency and cost of screening (annual and biennial); and background smoking-cessation rates. The scenarios were also evaluated by assessing the additional benefits and costs of coupling a smoking cessation program with the screening program.Footnote 9Footnote 10
OncoSim is led and supported by the Canadian Partnership Against Cancer, with model development by Statistics Canada, and is made possible through funding from Health Canada. OncoSim was formerly called the Cancer Risk Management Model or CRMM.
Modelling chronic disease: The Population Health Model (POHEM)
The Population Health Model (POHEM) is an empirically grounded, longitudinal microsimulation model of diseases and risk factors representing the life cycle dynamics of the Canadian population.Footnote 11 Reliably projecting the incidence and prevalence of conditions such as diabetes, osteoarthritis and cardiovascular disease, as well as multivariate mortality, requires a fully validated set of dynamic risk factor modules for smoking, body mass index, cholesterol and hypertension.Footnote 12
Physical activity is one of the risk factors that is simulated. The physical activity model was developed using the longitudinal National Population Health Survey and validated against subsequent years of the Canadian Community Health Survey. It includes walking and biking for transportation, leisure time physical activity, and an overall measure of physical activity, jointly estimated with a range of other risk factors (age, sex, region, ethnicity, alcohol, smoking, education and income, and body mass index) and self-reported chronic conditions (arthritis, cancer, hypertension, diabetes and heart disease) as well as health status and mortality.Footnote 13
The physical activity model, developed by Statistics Canada, was jointly funded by the Public Health Agency of Canada and Statistics Canada.
Modelling dementia: POHEM Neuro
Dementia places a heavy burden on caregivers and health care systems. Therefore, projecting its likely prevalence is useful for policy makers. A microsimulation model of dementia and other neurological conditions was developed as part of Canada's National Population Health Study of Neurological Conditions. The number of people living with dementia was projected to nearly double between 2011 and 2031. Likewise, the direct health care costs for people with dementia was projected to double from about $9.2 billion in 2011 to $18.2 billion in 2031.Footnote 14
The POHEM Neuro model was developed by Statistics Canada and funded through the Government of Canada's National Population Health Study of Neurological Conditions.
Where are we going next?
Increasingly, and appropriately, policy makers are required to use evidence-based evaluations of costs and benefits when deciding whether to implement new medical and non-medical interventions. Many of the most important health policy questions—for instance, trends in cardiovascular disease, cancer, dementia, cannabis and opioid use—are challenging to examine, and therefore require robust and comprehensive planning models.
Furthermore, Canada and other developed countries are faced with aging populations that will require more health care resources. Population aging and worsening health attributes, like obesity, may be contributing to a rise in chronic disease prevalence and health care system costs. Dynamic microsimulation is a useful methodology for investigating complex health and health system problems; it provides policy makers with a chance to foresee and explore the potential impacts of policy changes.
Future work in microsimulation modelling at Statistics Canada will include addressing some extremely complex health problems in collaboration with our partners. For instance, we are currently working to update the way cardiovascular disease—a leading cause of death and disability—is modelled by taking advantage of newly linked data. We have also begun preliminary investigative work to evaluate the feasibility of developing microsimulation models for cannabis and opioid use, their associated costs and potential harms. We also plan to expand our current dementia model to incorporate risk factors like smoking and alcohol intake.
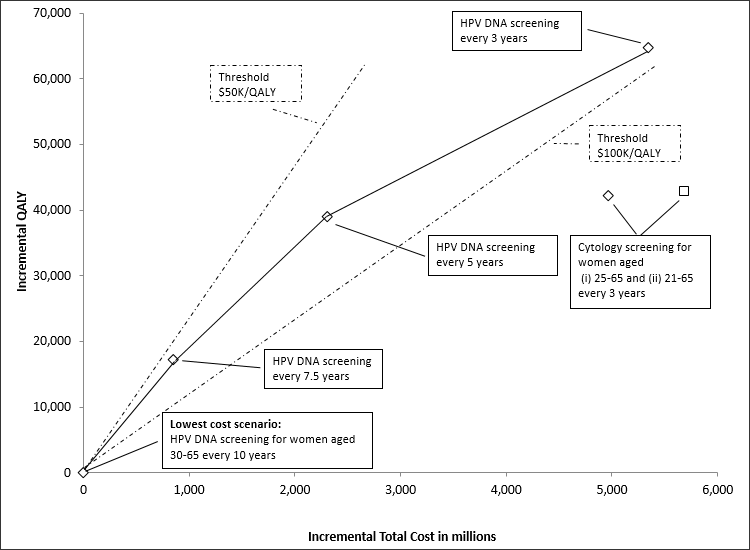
Figure 1 – Efficiency frontier: plot of incremental cost and quality adjusted life-years (QALYs) relative to lowest-cost scenario. (HPV = human papillomavirus, DNA = deoxyribonucleic acid)
| Scenario | Incremental cost | Quality adjusted life-years (QALY) |
|---|---|---|
| HPV DNA screening for women aged 30-65 every 10 years (Lowest cost scenario) | $0 | 0 |
| HPV DNA screening for women aged 30-65 every 7.5 years | $855,457,176 | 17,313 |
| HPV DNA screening for women aged 30-65 every 5 year | $2,310,537,663 | 39,074 |
| HPV DNA screening for women aged 30-65 every 3 years | $5,347,158,070 | 64,748 |
| Cytology screening for women aged 25-65 every 3 years | $4,965,726,990 | 42,141 |
| Cytology screening for women aged 21-65 every 3 years | $5,684,380,298 | 42,819 |
|
Notes:
|
||
Login/register to post comments.
Recent posts
-
 1904 people recommended this
1904 people recommended this -
 2551 people recommended this
2551 people recommended this -
 2925 people recommended this
2925 people recommended this
User comments
Great article!