

For the first time in more than 15 years, new data from the Canadian Health Measures Survey (CHMS), collected from November 2022 to December 2024, provide direct measures of oral health among Canadians, highlighting both improvements and ongoing challenges.
Direct measures provide objective assessments of oral health conditions, offering more accurate information than what is captured through self-reports and contributing to a more comprehensive understanding of the oral health of Canadians.
Results show that fewer seniors aged 60 to 79 years experienced complete tooth loss (edentulism) in 2022–2024 compared with 15 years earlier. The proportion of people aged 60 to 79 years with no natural teeth decreased from about 1 in 5 seniors (22%) in 2007–2009, the last time direct oral health measures were collected in the CHMS, to fewer than 1 in 10 seniors (8%) in 2022–2024. Despite this improvement, the prevalence and severity of dental caries (tooth decay) were unchanged from 2007–2009. Additionally, signs of gum inflammation remained common among Canadians aged 20 to 79 years, with 83% showing bleeding gums in 2022–2024, an important early sign of gum disease.
Among children aged 6 to 11 years, the prevalence and severity of dental caries in 2022–2024 were relatively stable compared with 2007–2009, with more than half (57%) having at least one affected primary or permanent tooth.
Tooth decay is unchanged among children, youth and adults
The decayed, missing and filled teeth (DMFT) index, which counts the number of decayed (D), missing due to decay (M) and filled (F) teeth (T), is commonly used to assess dental caries and treatment needs. It reflects the average number of affected teeth per person, indicating the overall severity of the problem. It is often used alongside prevalence, which measures the proportion of people with at least one affected tooth, to capture both how common dental caries is and how severe it is within a population.
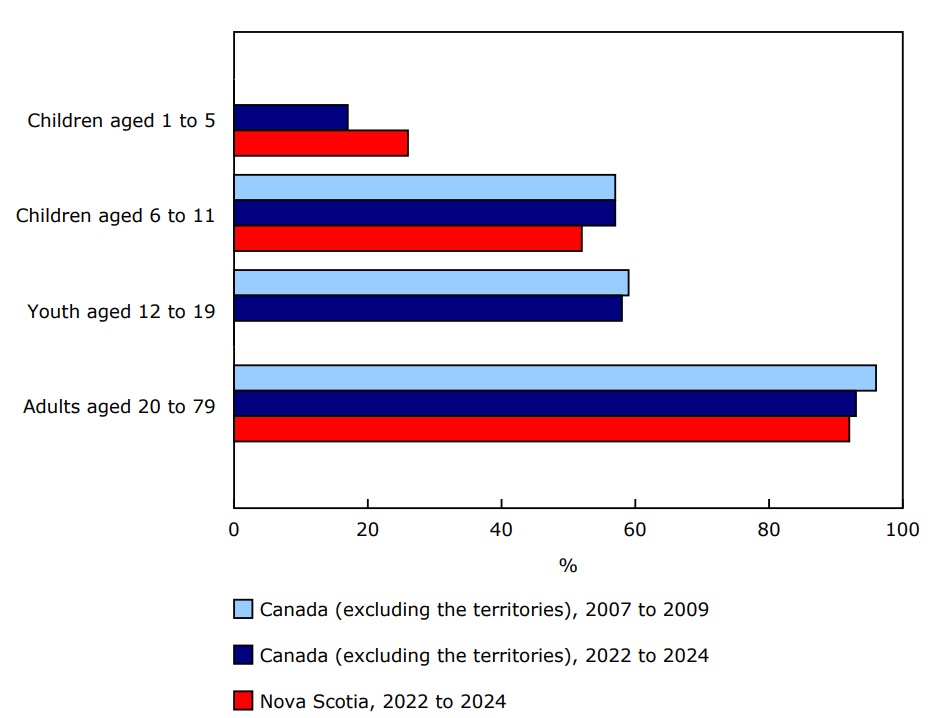
In 2022–2024, tooth decay was measured among children aged 1 to 5 years for the first time. In this group, 17% had at least one primary tooth affected, providing a baseline for future monitoring. Early tooth decay can progress quickly and is often associated with pain, difficulties in eating and increased risk of future dental complications. The presence of decay in this age group highlights the importance of prevention starting in the first years of life.
Among children (6 to 11 years) and youth (12 to 19 years), the proportion with at least one affected tooth showed no statistically significant changes from the 2007 to 2009 cycle of the CHMS to the 2022 to 2024 cycle. In 2022–2024, just over half (57%) of children aged 6 to 11 years had at least one affected primary or permanent tooth, consistent with the prevalence reported in 2007–2009 (57%). Similarly, 58% of youth had at least one permanent tooth affected in 2022–2024, compared with 59% in 2007–2009. The average number of affected teeth was also similar among children (2.4 teeth) and youth (2.3 teeth), with no significant changes over time.
While the prevalence of tooth decay in children and youth was stable in 2022–2024, more than half of children and youth had dental caries, highlighting that challenges remain.
Among adults (aged 20 to 79 years), the percentage with at least one affected permanent tooth was consistent, at 96% in 2007–2009 and 93% in 2022–2024. The average number of affected teeth was also stable, at 10.7 in 2007–2009 and 9.7 in 2022–2024.
Measuring the consequences of untreated tooth decay
In 2022–2024, the survey gathered information for the first time on the pulp, ulceration, fistula and abscess (PUFA) index, which identifies teeth with advanced consequences of untreated decay: visible pulpal involvement (the inner part of the tooth) (P), ulceration caused by dislocated tooth or root fragments (U), fistula (F) or abscess (A). While the DMFT index reflects overall experience with dental caries, the PUFA index highlights the severity and complications resulting from untreated tooth decay.
In 2022–2024, PUFA affected 7% of children and youth aged 1 to 19 years and 22% of adults aged 20 to 79 years, highlighting the ongoing burden of advanced disease across all ages. Monitoring PUFA can help identify populations most in need of urgent dental care and guide targeted efforts to prevent serious complications.
Changes in gum pockets depths in adults
Periodontal disease develops when the tissues and bone supporting teeth become damaged, often due to bacteria and inflammation. A key method for evaluating gum health in adults is measuring the depth of space between the teeth and the gum, known as the sulcus or pocket, using a procedure called periodontal probing. As gum disease progresses, these pockets deepen due to ongoing inflammation and breakdown of supporting tissue. Probing depths of up to 3 mm are generally considered healthy, while deeper pockets may indicate early signs of gum disease.
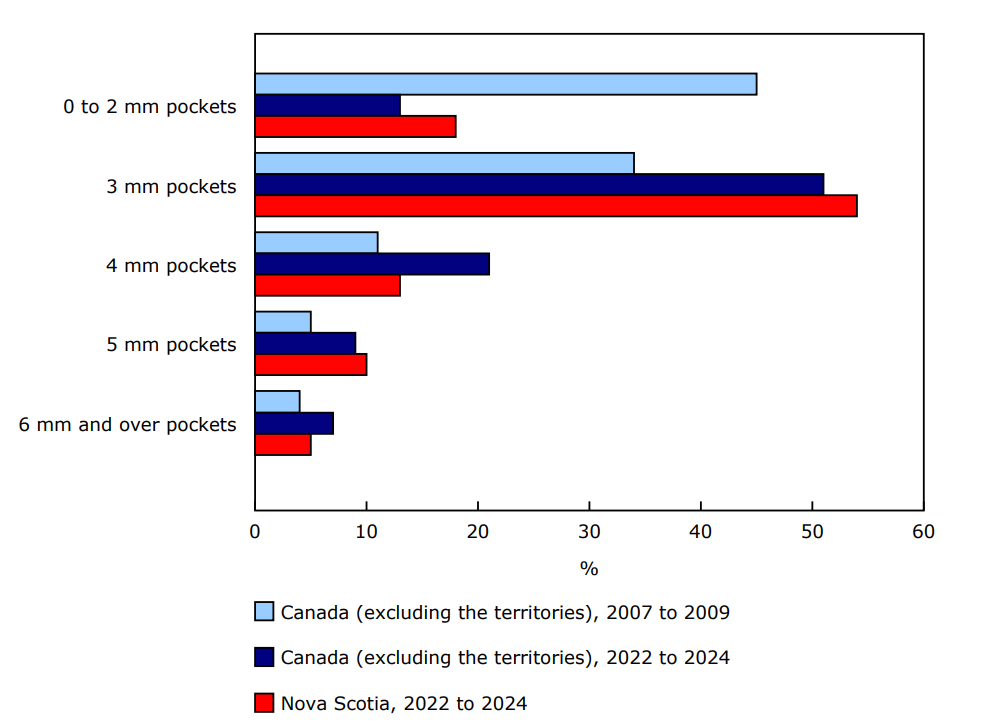
From 2007–2009 to 2022–2024, pocket depths in adults aged 20 to 79 years changed. The percentage of adults with pocket depths of 0 to 2 mm declined from 45% to 13%; conversely, the prevalence of 3 mm pocket depth increased from 34% to 51%. At the same time, deeper pockets became more common. Indeed, the prevalence of 4 mm pockets increased from 11% to 21% and that of 5 mm pockets was up from 5% to 9%. No statistically significant differences were observed in the prevalence of pockets 6 mm or over (4% in 2007–2009 and 7% in 2022–2024). Although the pocket depths of close to two-thirds of adults were in the healthy range (0 mm to 3 mm) in 2022–2024, just over one-third had deeper pockets (4 mm and over) compared with one in five adults in 2007–2009.
This shift toward deeper periodontal pockets appears to be in line with international trends. Recent studies from the United Kingdom and Australia reported an increasing burden of periodontal disease, with both prevalence and severity expected to rise. These patterns are linked to limited access to preventive dental care, high treatment costs, unequal insurance coverage and socioeconomic challenges. In Canada, gaps in early intervention, combined with persistent access and coverage challenges since 2007–2009, may be contributing to the increase in prevalence and severity.
Gum inflammation is relatively common, especially among young adults
While pocket depth provides information about structural changes associated with gum disease, bleeding on probing reflects active inflammation and offers additional insight into the current activity of the disease.
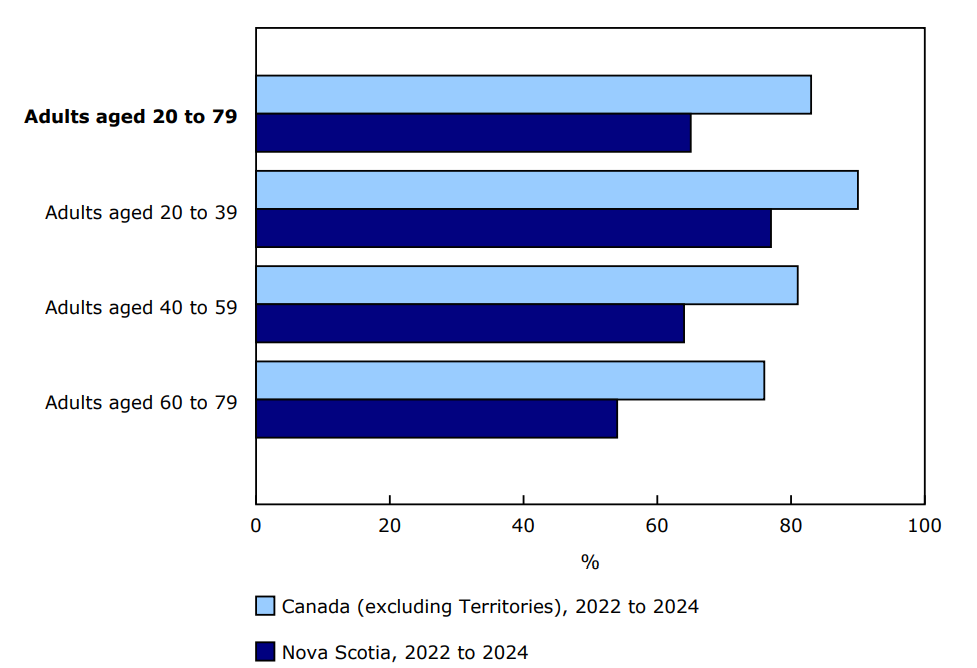
Overall, among Canadians aged 20 to 79 years, the average number of teeth with bleeding in 2022–2024 was seven, with 83% of people showing gum bleeding in at least one tooth during probing. Rates were highest among people aged 20 to 39 years (90%) and lowest among those aged 60 to 79 years (76%). These results suggest that inflammation is relatively common in certain age groups, especially among young adults (aged 20 to 39 years), highlighting the importance of improving oral hygiene practices and access to dental care among this population.
Declines in complete tooth loss among Canadian adults
The rate of edentulism among adults aged 20 to 79 years declined from 6% in 2007–2009 to 3% in 2022–2024. Among seniors aged 60 to 79 years, rates dropped from 22% to 8% during the same period. These declines likely reflect improvements in dental care and a gradual shift in treatment practices over recent decades, from extraction-focused approaches toward preserving natural teeth whenever possible. Despite these positive changes, edentulism rates among seniors remain higher than among adults aged 20 to 59 years, pointing to age-related differences in oral health.
First provincial Canadian Health Measure Survey data are available in support of Nova Scotia's oral health surveillance program
With data collection being expanded to five additional sites through a special collaboration with Nova Scotia Department of Health and Wellness, oral health estimates based on direct measures collected in the CHMS are available at the provincial level for the first time with this release.
Overall, results show that oral health outcomes in Nova Scotia were closely aligned with national results. In 2022–2024, among adults aged 20 to 79 years, the average DMFT score was 9.2 in the province, compared with 9.7 nationally, and 92% had at least one affected tooth, compared with 93% across Canada. The average number of untreated coronal cavities among adults was 2.5 in Nova Scotia, similar to the national average of 2.9. For periodontal health, the average pocket depth for adults aged 20 to 79 years was 5 mm (national average: 5 mm), while 65% of individuals aged 20 to 79 years exhibited bleeding on probing (national prevalence: 83%).
These findings suggest that oral health challenges in Nova Scotia are similar to those observed at the national level. Building on these findings, Nova Scotia plans to further analyze the data to inform provincial policy and program decisions, providing a basis for tailoring prevention and treatment efforts to the needs of the population.
Chart 1: Prevalence of tooth decay among the dentate population aged 1 to 79 years in Nova Scotia and Canada (excluding the territories)
Description - Chart 1
Notes: There are no statistically significant differences between Canada (excluding the territories) and Nova Scotia for the period of 2022 to 2024. Similarly, no statistically significant changes were observed from 2007–2009 to 2022–2024 for Canada (excluding the territories). Prevalence of tooth decay refers to the proportion of individuals with at least one affected tooth, measured by the number of decayed (D), missing due to decay (M) and filled (F) teeth (T), using the DMFT index. Data for children aged 1 to 5 years include only primary teeth (dmft), those for children aged 6 to 11 years include primary and permanent teeth (dmft + DMFT), those for youth and adults aged 12 to 79 years include only permanent teeth (DMFT) and those for adults aged 20 to 79 years refer to the crown only. For Nova Scotia estimates, results for children aged 1 to 5 years and children aged 6 to 11 years are flagged as "E" and should be used with caution.
… Not available for this time period
F too unreliable to be published
Sources: Canadian Health Measures Survey – Cycle 1 (2007 to 2009) and Cycle 7 (2022 to 2024) (5071).
Chart 2: Prevalence of periodontal pockets by highest score among the dentate population aged 20 to 79 years in Nova Scotia and Canada (excluding the territories)
Description - Chart 2
Notes: There are no statistically significant differences between Canada (excluding the territories) and Nova Scotia for the period of 2022 to 2024. Prevalence of periodontal pockets by highest score refers to the proportion of individuals classified according to the deepest pocket measured in their mouth.
Sources: Canadian Health Measures Survey – Cycle 1 (2007 to 2009) and Cycle 7 (2022 to 2024) (5071).
Chart 3: Prevalence of gum bleeding on probing among the dentate population aged 20 to 79 in Nova Scotia and Canada (excluding the territories)
Description - Chart 3
Notes: There are no statistically significant differences between Canada (excluding the territories) and Nova Scotia for the period of 2022 to 2024. Prevalence of gum bleeding on probing refers to the proportion of people with gum bleeding in at least one tooth during probing. For Nova Scotia estimates, results for adults aged 20 to 39 years, 40 to 59 years and 60 to 79 years are flagged as "E" and should be used with caution.
Sources: Canadian Health Measures Survey – Cycle 1 (2007 to 2009) and Cycle 7 (2022 to 2024) (5071).
Note to readers
The Canadian Health Measures Survey (CHMS) is the only ongoing nationally representative source of direct health measures in Canada. It provides detailed insight into the health conditions and behaviours of the Canadian population and is designed to inform the prevention, diagnosis and treatment of illnesses, as well as to promote health and wellness.
Data for cycle 7 of the CHMS were collected from November 2022 to December 2024. The target population included persons aged 1 to 79 years living in the 10 provinces. The observed population excludes persons living in the three territories, persons living on reserves and other Indigenous settlements in the provinces, full-time members of the Canadian Forces, the institutionalized population and residents of certain remote regions. Altogether, these exclusions represent approximately 3% of the target population.
The CHMS cycle 7 marks the first time since cycle 1 (2007 to 2009) that oral health data were collected through direct measurements.
The CHMS Nova Scotia oral health data combine data from one collection site (Halifax) from cycle 7 of the CHMS, as well as data collected at five additional sites across the province from November 2024 to March 2025. This is the first time that a provincial data file is available from the CHMS, as the data collection and weighting were specifically designed to generate provincial estimates.
All estimates related to dental caries and gum health presented in this release are based on the dentate population (individuals with at least one natural tooth).
For adults aged 20 to 79 years, the decayed, missing and filled teeth (DMFT) index presented in this release refers to the crown only.
Dental caries refers to the process of tooth decay, including early stages of weakened enamel to deeper decay affecting the areas below the enamel (dentin and pulp). In early stages, caries can be reversed with treatment or improved oral hygiene practices.
A cavity is a physical hole in the tooth that results from advanced caries. It typically requires professional intervention (e.g., fillings or crowns).
Probing is used to measure periodontal pocket depth, which is the distance from the gum margin (free gingival margin) to the bottom of the gum or periodontal pocket. Probing is performed on all tooth surfaces to the nearest millimetre using a standardized, graduated periodontal probe. In addition to depth, probing can also detect bleeding on probing, which is an important indicator of gum inflammation.
In CHMS cycle 7, periodontal pocket depths were measured using direct dental probing to assess gum health in adults. The examiners were trained and calibrated to improve consistency and reduce measurement error. Nevertheless, as with any large-scale study, minor measurement errors and potential biases may still occur and should be considered when interpreting population-level results.
Contact information
For more information, or to enquire about the concepts, methods or data quality of this release, contact us (toll-free 1-800-263-1136; 514-283-8300; infostats@statcan.gc.ca) or Media Relations (statcan.mediahotline-ligneinfomedias.statcan@statcan.gc.ca).