

Today, Statistics Canada is releasing data from a new crowdsourced study, Living with a Life-Limiting Illness: Access to Care and Related Experiences, collected from October 8, 2024, to March 31, 2025. The purpose of this study is to better understand the lived experience of Canadians who are affected by diseases or conditions that cannot be cured, get worse over time and ultimately shorten their lifespan. It also aims to provide information on the experience of Canadians who act as unpaid caregivers in a non-professional capacity—such as family, friends or community members—to those with life-limiting illnesses.
As Canada's population ages and the number of individuals living with life-limiting illnesses increases, the demand for high-quality palliative care continues to grow. Understanding the barriers and supports related to access is critical to ensuring that Canadians receive timely and appropriate care. Such care can reduce suffering, improve quality of life and extend survival.
This release highlights key findings from a crowdsourced study on timely access to care, barriers to care and factors affecting care for persons living with life-limiting illnesses and their unpaid caregivers. As the results from this study were gathered through crowdsourcing, they are not expected to be representative of the population and should be interpreted with caution. More details about the methods used in this crowdsourced study can be found in the Note to readers below.
Portrait of study participants
Of all study participants (984 participants), over one-third (36%) identified as persons living with a life-limiting illness in 2024, while nearly two thirds (64%) identified as unpaid caregivers (Table 1). Among those living with a life-limiting illness, most (69%) reported having an unpaid caregiver. When asked about the nature of their caregiving relationships, the most common response was that the caregiver was a spouse, common-law partner or partner (39%), followed by a child (31%) and a parent (9%).
Women represented 59% of participants living with a life-limiting illness, while men accounted for 41%. Among unpaid caregivers, more than three-quarters (77%) identified as women, whereas 23% identified as men. This aligns with broader caregiving trends in Canada, in which women are more likely than men to take on caregiving responsibilities.
When asked about the most impactful illness they were living with, nearly one-third (30%) of participants reported it being advanced cancer, followed by dementia or Alzheimer's disease (18%) and neurological conditions (16%), including amyotrophic lateral sclerosis (or Lou Gehrig's disease), multiple sclerosis, Parkinson's disease and Huntington's disease.
The majority (83%) of participants resided in a private home or apartment, and nearly half (47%) of all participants expressed a preference for receiving end-of-life care in these settings. The supportive environment of a hospice (21%) or long-term care facility (6%) emerged as the next most preferred settings. Additional characteristics of the study participants are provided in Table 1.
Older adults and persons with advanced cancer report having higher levels of palliative care
A palliative approach focuses on improving quality of life for people living with serious illnesses and their families. It is holistic, addressing physical, emotional, social and spiritual needs, and can be provided alongside active treatment and not solely at the end of life. Key components include timely access to care, clear communication with providers, effective pain and symptom management, care planning and culturally sensitive support.
This study asked a series of questions to the participants to understand their palliative care experience. Results from these questions were then used to create a summary score representing the level of palliative care received. To define the level of palliative care, responses to these questions were combined and categorized into a three-scale range: high, moderate and low. The high level represents persons with a life-limiting illness who have received most elements of a palliative approach to care. Among all participants, in 2024, 27% reported experiencing a high level of palliative care, 43% experienced a moderate level and 30% experienced a low level (Table 2). Care experiences varied across age groups: 32% of participants aged 65 years and older reported receiving a high level of palliative care, compared with 25% of those aged 45 to 64 years and 13% of those aged 15 to 44 years.
Among the three most reported health conditions, advanced cancer had the highest proportion of participants who received a high level of palliative care (42%). This aligns with findings from administrative data across hospitalization, home care and long-term care settings, which show that patients with cancer have better access to palliative care than those with other conditions. Dementia or Alzheimer's disease had the highest proportion of participants who received a low level of care (38%). Responses from participants with neurological diseases were more distributed across care levels, with the highest proportion of these participants reporting a moderate level of care (46%). Additional information on the level of palliative care received by study participants, by gender, provincial region and area of residence, is provided in Table 2.
Majority of participants report difficulty accessing health care services outside regular hours
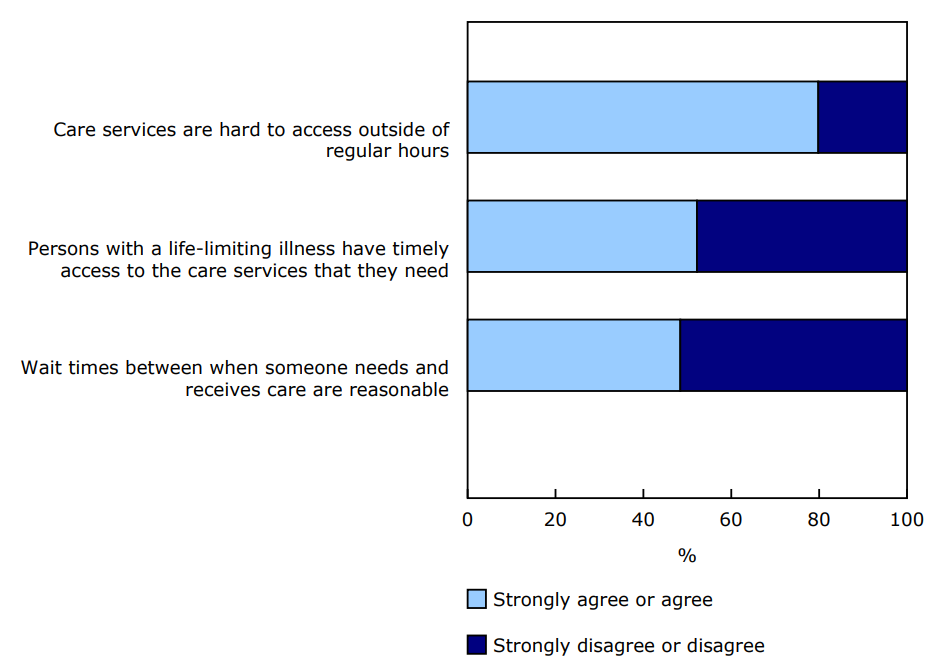
When asked about timely access to care in 2024, just over half (52%) of participants strongly agreed or agreed that persons living with a life-limiting illness generally have timely access to the care services that they need. However, the majority (80%) of participants strongly agreed or agreed that health care services were hard to access outside of regular hours, such as overnight, on weekends or during holidays (Chart 1). The top three services that participants had difficulty accessing at the time they needed it were pain and symptom management (36%), referral to specialists (35%) and care coordination (31%) (Table 3). Participants aged 65 years and older identified respite care for caregivers (29%) as a service they had difficulty accessing in times of need.
There were differences in perceptions of timely access to care based on age. Participants in the oldest age groups shared similar opinions on timely access to care, with more than half of persons aged 45 to 64 years (54%) and those aged 65 years and older (55%) having strongly agreed or agreed that they generally have timely access to the care service that they need. In contrast, one-third (34%) of persons aged 15 to 44 years strongly agreed or agreed that they generally had timely access to care that they need.
The top three factors that impacted participants' ability to access care promptly were the availability of care providers or specialists (71%), difficulty navigating the health care system (45%) and availability of services in their preferred care setting (37%) (Table 4).
Over half of participants report having complications due to delayed support for serious illness
Measuring the impact of a lack of timely support, especially in palliative care, is vital because it reveals how delays or gaps in care affect patients, caregivers and the health care system as a whole.
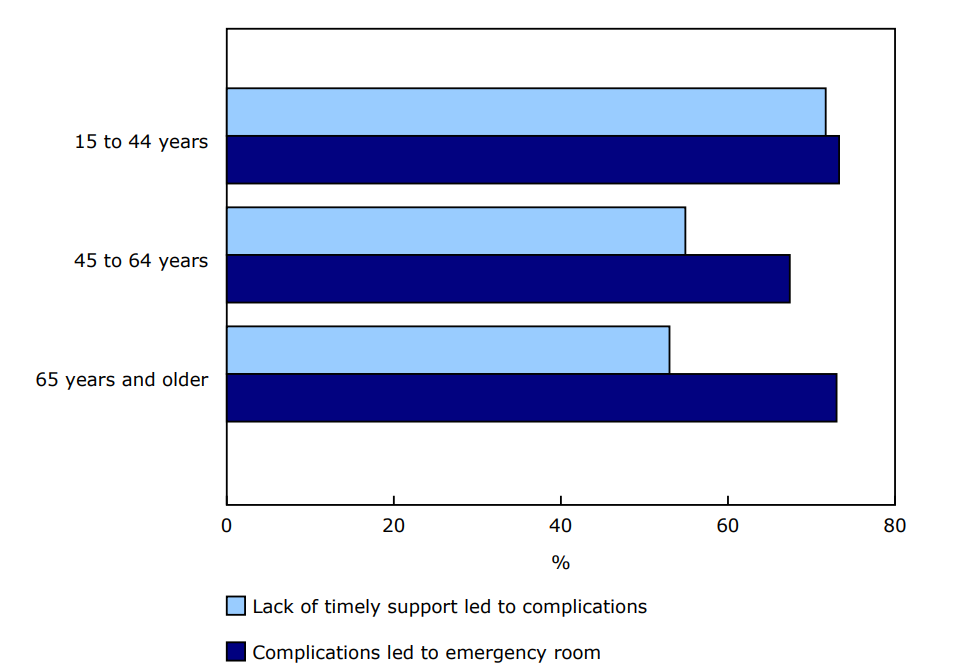
More than half of men (52%) and women (59%) in 2024 stated that there have been situations where the lack of timely support for their serious illness led to unexpected, self-reported complications. Participants aged 15 to 44 years (72%), 45 to 64 years (55%) and 65 years and older (53%) all reported experiencing situations where delayed or insufficient support worsened their conditions (Chart 2).
A substantial proportion (71%) of participants reported visiting the emergency room in the year preceding data collection. Both men (74%) and women (70%), as well as individuals from all age groups, from 15 to 44 years (73%), 45 to 64 years (67%) and 65 years and older (73%), faced similar challenges in navigating the health care system, often resulting in urgent visits to the emergency room. These experiences, while important, are self-reported and drawn from a self-selected group and may not reflect the experience of the general population.
Most unpaid caregivers do not have their support needs assessed
Identifying and understanding which forms of support are most beneficial for unpaid caregivers is essential for building a compassionate, efficient and equitable health care system that provides support and improves the well-being of caregivers as well as improves the quality of life of persons living with life-limiting illnesses.
Support for unpaid caregivers may include services such as training, support groups, home care and temporary respite care for the person they care for. These types of support may be identified through caregiver assessments, which are sometimes conducted by health or social service professionals to help determine what assistance a caregiver might need in their role. Among unpaid caregivers who participated in the study in 2024, the top three areas where they felt more support would have been the most beneficial were enhanced communication with health care providers (36%), respite care (35%) and both professional homecare services and financial support (31%) (Table 5). Moreover, the majority (89%) of unpaid caregivers reported not having an assessment to determine their needs for support in their caregiving role.
When it came to the support unpaid caregivers did receive, the responses were somewhat mixed. Overall, about half (49%) of unpaid caregivers reported receiving at least partial support, such as access to services or assistance, in their caregiving efforts. Even if they received some support, it was not always enough to meet the full scope of their needs. In comparison, 39% of unpaid caregivers stated they received no help at all.
Chart 1: Proportion of crowdsourced participants reporting agreement with statements about timely access to care, 2024
Description - Chart 1
Note: All estimates should be used with caution due to the limitations of crowdsourced studies.
Source: Living with Life-Limiting Illness: Access to Care and Related Experiences, October 8, 2024, to March 31, 2025 (5416).
Chart 2: Proportion of crowdsourced participants reporting complications due to lack of timely support and subsequent emergency room visits, by age group, 2024
Description - Chart 2
Note: All estimates should be used with caution due to the limitations of crowdsourced studies.
Source: Living with Life-Limiting Illness: Access to Care and Related Experiences, October 8, 2024, to March 31, 2025 (5416).
Note to readers
This release is based on the crowdsourcing initiative Living with a Life-Limiting Illness: Access to Care and Related Experiences . This crowdsourced study was developed by Statistics Canada in collaboration with Health Canada, the Canadian Institute for Health Information and the Public Health Agency of Canada.
Acknowledging respondent participation
Statistics Canada acknowledges the valuable contribution of study participants, particularly given the sensitive nature of the subject matter. The participation of individuals living with life-limiting illnesses and their unpaid caregivers has enabled the collection of new and important data on palliative care experiences across Canada.
Methodology
This crowdsourced study for the first time reached out to individuals living with life-limiting illnesses and their unpaid caregivers. Participants living with a life-limiting illness were asked a series of questions about their health care experience. Unpaid caregivers were also asked to report on the experience of the person that they provided care for. To support a comprehensive analysis, responses from the questions that were asked to both persons living with life-limiting illnesses and unpaid caregivers were combined. Caregiver-specific questions were answered exclusively by unpaid caregivers.
Crowdsourcing is a method of collecting information from a community of individuals, where they voluntarily provide valuable data for statistical purposes. Statistics Canada uses crowdsourcing to collaborate with stakeholders and citizens. It relies on the principle that individual citizens are experts within their local environments. However, because participation is open and voluntary, crowdsourced data are not statistically representative of the Canadian population. For more information, see Statistics Canada's resource on non-probability sampling.
While several administrative databases at the national and provincial levels provide data on hospitals, home care and long-term care facilities, there is currently no systematic enumeration of individuals living with life-limiting illnesses in Canada, specifically those residing in communities. In areas where no existing sampling frame is available, crowdsourcing provides a practical approach to gathering experiential information directly from those affected. This helps address data gaps in emerging or under-researched topics.
Canadian residents aged 15 years or older living with a life-limiting illness or unpaid caregivers of persons living with a life-limiting illness in the two years preceding data collection were invited to complete the online questionnaire from October 8, 2024, to March 31, 2025. Nearly 1,000 individuals from the provinces and territories filled out the crowdsourcing questionnaire: 352 persons (36%) were living with a serious illness and 632 (64%) were unpaid caregivers for a person with a serious illness.
The questionnaire was designed to capture a wide range of experiences and perspectives and was structured into two distinct question streams: one for individuals living with a life-limiting illness and another for unpaid caregivers of those living with a life-limiting illness. Unpaid caregivers answered questions about the care of the person with a life-limiting illness as well as questions about their own experiences of supportive care for themselves. Results from both sources were combined wherever appropriate for the purpose of this analysis.
Participation in the study was encouraged with various promotional efforts, including recruitment of partner organizations to help promote the study Call for Collaboration - Living with a Life-limiting Illness: Access to Care and Related Experiences, the development of a promotional toolkit, reminders to organizations to promote the ongoing study throughout collection, a social media campaign and stakeholder emails asking for help to promote the study. Contact with individuals with a life-limiting illness or unpaid caregivers of those living with a life-limiting illness in the two years preceding the data collection was principally via partner organizations involved in providing services to these populations.
The results obtained from the crowdsourced study pertain only to the participants and cannot be used to draw conclusions about the general Canadian population. As crowdsourcing collects data from self-selected volunteers, the data are subject to multiple biases. Differences between groups may reflect participation patterns rather than actual differences in care experiences across the population. It was not possible to calibrate results to the Canadian population as there are no reliable population counts for those living with a life-limiting illness.
As crowdsourcing is based on a non-probability sample, measures of sampling error such as variance, coefficients of variation, margins of error and confidence intervals cannot be calculated. In the absence of a sampling framework, selection probabilities were not defined and survey weights were not calculated. Additionally, no adjustment was made for non-response, as the concept of a non-response rate is not applicable to crowdsourced data. While this study provides valuable qualitative insights, results should be interpreted with appropriate caution.
Concepts and definitions
A palliative care approach is a specialized form of medical care for people with serious illnesses. It focuses on providing relief from symptoms and concerns, with the goal of improving quality of life for both the person with a serious illness and their family and unpaid caregivers. It is a holistic approach that addresses physical, emotional, social and spiritual needs and can be provided alongside treatment for the serious illness. Palliative care can be beneficial at any point in a person's illness, not just at the end of life. Note that the study avoids using the term "palliative care" in the questionnaire and instead refers to the supportive care received since diagnosis of a life-limiting illness. This decision was made as the term "palliative care" is not well understood.
The "level of palliative care" measure is a derived summary score based on responses to 16 questions related to key elements of a palliative approach to care. Key components include timely access to care, clear communication with providers, effective pain and symptom management, care planning and culturally sensitive support. To view the questions used to create the derived summary score, visit the Living with a Life-Limiting Illness: Access to Care and Related Experiences, 2024 questionnaire. Results from these questions were then used to create a derived measure representing the level of palliative care received. Respondents were assigned to one of three levels: low (0 to 5 points), moderate (6 to 10 points) or high (11 to 16 points) based on their reported experiences and access. The high level represents persons with a life-limiting illness who have received most elements of a palliative approach to care. This is not a validated clinical indicator, and the results reflect only the experiences of those who voluntarily participated in the study. The variables used to calculate this measure were aligned with the Quality Standards for Palliative Care developed by Ontario Health and Health Quality Ontario.
The derived measure does not reflect all aspects of a palliative approach to care but was designed to provide an overview of the level of care received as measured through the study questions and where the survey design allowed. For example, the derived measure does not include experiences related to care transitions between settings (e.g., from hospital to home), which is an important component of quality palliative care but was excluded due to survey design limitations.
Differences between groups may be influenced by participation patterns or response bias, rather than reflecting actual differences in care experiences across Canada.
The concept of rurality was defined using Statistics Canada's Population Centre and Rural Area Classification. A population centre has a population of at least 1,000 and a population density of 400 persons or more per square kilometre, based on population counts from the 2021 Census of Population. All areas outside population centres are classified as rural areas.
Contact information
For more information, or to enquire about the concepts, methods or data quality of this release, contact us (toll-free 1-800-263-1136; 514-283-8300; infostats@statcan.gc.ca) or Media Relations (statcan.mediahotline-ligneinfomedias.statcan@statcan.gc.ca).